Case Report Published on December 28, 2024
Primary Aspergillosis of the Vocal Cord: A Case Report
Ruksana H1, Darshana Ravindran1, Santhi T1
1. Government TD Medical college, Alappuzha, Kerala*
ABSTRACT
Primary Aspergillosis of the larynx is very rare, and it usually mimics a malignant or pre-malignant lesion. Hence, it is important for us to be aware of this condition to avoid misdiagnosis and treatment delay. A case of primary aspergillosis of the vocal cord is reported in this article. The clinical manifestations and treatment modalities are also discussed.
Keywords: Primary, Aspergillosis, Larynx, Antifungals
INTRODUCTION
Aspergillosis is an infection caused by the fungus Aspergillus. Aspergillosis primarily affecting the larynx is very rare. Larynx is usually involved secondarily. The lesion can be confined to the vocal cord or can involve the other sites of the larynx. The lesion of aspergillosis can mimic malignancy or a pre malignant condition.1 Some of the risk factors which predispose to the condition include the use of corticosteroids and the immunocompromised state of the body. Direct laryngoscopic examination showing whitish irregular surfaced lesion R vocal cord. (Figure 1).
The condition usually responds well to antifungals. Here we are reporting a case of primary aspergillosis of the vocal cord in a patient without any underlying risk factor. Histopathology examination showing septate dichotomously branching hyphae (Figure 2).
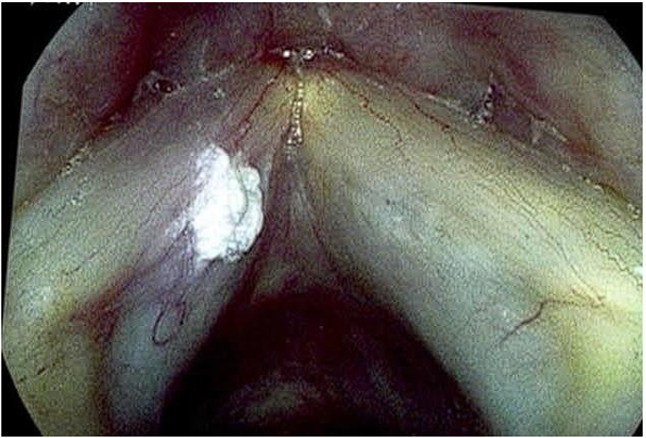
Figure 1. Endoscopic examination

Figure 2. Histopathology
CASE REPORT
A 70-year-old male patient presented with progressive hoarseness of 8 months duration. He was from a rural area and a farmer by profession. There was no associated dysphagia, foreign body sensation of the throat, breathing difficulty, or voice abuse. There was no history of diabetes mellitus, use of any immunosuppressive medications, malignancy, bronchial asthma or history of any surgeries in the past. There was no history of any addictions.
The patient was of moderate built and nourishment. General physical examination was normal. All the routine blood examinations were normal, and he was seronegative for HIV, anti-HCV and HBsAg. A 70-degree endoscopic examination was done, which showed a whitish irregular surfaced lesion involving the medial and superior surface of the right vocal cord, between the junction of anterior one-third and posterior two thirds.
Microlaryngeal excision of the lesion was done and the specimen on histopathological examination showed fungal hyphae consistent with Aspergillus.
The patient was treated postoperatively with the anti-fungal, oral itraconazole 100 mg once daily for 4 weeks. His voice improved. A 70- degree endoscopy was done 4 weeks later which showed apparently normal vocal cords. A pulmonary medicine consultation was done to rule out any foci in the lungs. Sputum culture and sensitivity, and fungus staining were done. No fungal elements were detected. An X-ray of the chest was normal.
Bronchoscopy was done and the bronco alveolar lavage study did not detect any fungal element. Hence the case is consistent with primary aspergillosis of vocal cord in an immunocompetent patient, a very rare clinical entity.
DISCUSSION
Aspergillosis is a group of diseases caused by the fungus Aspergillus. Aspergillus species belongs to the Aspergillacea family. The most common ones causing human infection are Aspergillus fumigatus and Aspergillus Niger. Less common are Aspergillus nidulus, Aspergillus flavus and Aspergillus versicolor. Aspergillus is a genus that comprises more than 200 species and can be found as ubiquitous saprophytes growing in soil and decaying matter.
They may cause opportunistic infections like sinusitis, bronchitis, allergic broncho pulmonary aspergillosis, aspergilloma, and invasive aspergillosis. The severity of the infection depends upon host immunity. Because of high humidity and sunlight, fungal infections are more common in tropical areas. Conditions causing low body resistance like malignancy, diabetes, immunodeficient diseases, patients receiving cytotoxic drugs, steroids, broad-spectrum antibiotics and radiotherapy are prone to develop fungal infection.2 In the above-discussed case, none of these factors were present.
Aspergillosis is classified into superficial and deep infections. Superficial infection involves the mucosal lining. Deep infection involves the deeper tissues, which spread by blood dissemination to organs like the lungs, liver, heart, brain, kidneys, spleen, gastrointestinal tract, and lymph nodes.3 On histopathological examination, aspergillosis is classified into necrotizing, suppurative, and granulomatous.
Specimens collected from the patient for the diagnosis of aspergillosis include tissue, aspirates, and fluids like broncho-alveolar lavage. The tissue must be sent in a sterile tube or container and formalin fixed. Stains used for examination of fungal species include periodic acid Schiff (PAS), Gomori’s Methenamine Silver stain (GMS) and calcofluor white. Septate, dichotomous branching hyphae are observed. The histopathology of invasive fungal Aspergillosis shows pale necrotic mucosa as fungal angioinvasion causes infarction.
Management of primary laryngeal aspergillosis include systemic Amphotericin B, Itraconazole, and surgical stripping of the lesion.4 Our patient received 100mg of Itraconazole once daily for 4 weeks, with a good result.
END NOTES
Author information
- Dr. Ruksana H, Senior resident in ENT, Government TD Medical college, Alappuzha.
- Dr. Darshana Ravindran, Assistant Prof of ENT, Government TD Medical college, Alappuzha.
- Dr. Santhi T, Professor & Head of ENT, Govt TD Medical college, Alappuzha.
Conflicts of Interest: None declared.
Financial Support: Nil.
REFERENCES
- Klein AM, Tiu C, Lafreniere D. Malignant mimickers: chronic bacterial and fungal infections of the larynx. J Voice. 2005; 19: 151-7.
[Pubmed] - Athanassiadou F, Kourti M, Papageorgiou T, DanielidisInvasive J. Aspergillosis of the larynx in a child with acute lymphoblastic leukemia. Pediatr Infect Dis J. 2005; 24: 190-1.
[Pubmed] - D.L. Longo, A. Fauci, D.L. Kasper, J.L. Jameson, S.L. Hauser, J. Loscalzo. Harrison’s Principles of Internal Medicine(18th ed.), The McGraw-Hill Companies, Inc., USA (2012)
- Sambatakou H, Dupont B, Lode H, Denning DW. Voriconazole treatment for subacute invasive and chronic pulmonary aspergillosis. Am J Med. 2006; 119: 17-24.
[Pubmed]