Case Report Published on June 20, 2024
Mastoid Osteoma - A Rare, But Aesthetic Challenge!
Sree L1, M Suresh Kumar1
1. Department of Otorhinolaryngology, KIMS Health, Trivandrum*
ABSTRACT
Mastoid osteomas are benign, slow growing tumours arising in the temporal bone. Osteomas of the temporal bone are rare entity with incidence of about 0.1-1% of all benign tumours of skull. However only a few cases reported till date. Here we are reporting a rare case of mastoid osteoma, which due to cosmetic reasons managed surgically.
Keywords: Mastoid, Osteoma, Swelling, Temporal Bone
INTRODUCTION
Osteomas are benign outgrowth of bone. They are more common in the frontal and ethmoid sinuses. They are osteoblastic mesenchymal tumours1. Most of the cases are asymptomatic but can present with either external auditory canal obstruction or cosmetic problem. In the temporal bone, external auditory canal is the predominant location but presentation in the mastoid is rare. Although etiology is unknown in this case, causes of mastoid osteoma can be trauma, previous surgery, radiotherapy, chronic infection, hormonal factors etc. Incidence of mastoid osteoma is 0.1-1% and only few cases reported till date. Management of mastoid osteomas are indeed an aesthetic and surgical challenge. Herein we are reporting an aesthetically challenged case of mastoid osteoma, which we have managed successfully.
CASE REPORT
A 36 year old female presented with swelling behind the right ear, which she noticed around 12 years back (Figure 1). It was painless and gradually increasing in size. There was no history of trauma, hard of hearing, ear discharge, tinnitus, headache, cranial nerve deficit. There were no symptoms of inflammation of the swelling. No history of similar swelling in family. However due to cosmetic reasons, patient sought medical attention. On examination, a well-defined 3.5 x 3cm swelling noted over the mastoid region on the right side which is hard in consistency, non-tender, non-pulsatile, non-compressible, no rise in temperature over the swelling, no overlying skin changes and fixed. External auditory canal was normal and tympanic membrane was intact. Left ear, nose and throat were normal, no palpable neck nodes. Pure tone audiometry and tympanometry were normal. All routine laboratory tests were normal. Due to hard consistency, FNAC from the swelling was not possible.
HRCT Temporal bone was taken, which revealed a rounded bony lesion measuring 2x2x1.7cm noted from the right mastoid laterally in continuity with the cortex suggestive of osteoma. The middle ear cavity and mastoid air cells appear normal (Figure 2). Left mastoid was normal.
We had proceeded with surgical excision of the osteoma under general anaesthesia. Post auricular incision was placed and osteoma exposed completely after elevating the periosteum (Figure 3). Excision was done by drilling out (Figure 4) and detaching its attachment from mastoid using chisel and hammer (Figure 5). Specimen was sent for histopathological examination. Wound was sutured in layers. Post-operative period was uneventful. Histopathological studies showed a circumscribed neoplasm composed of cortical type bone pattern with haversian like canals, consistent with osteoma.
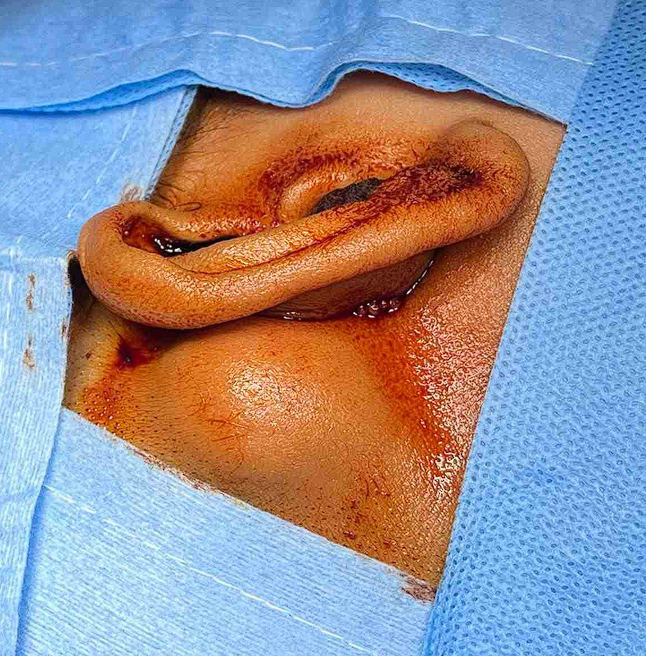
Figure 1. Pre-operative image of right mastoid osteoma

Figure 2. CT temporal bone image in multiple planes showing osteoma
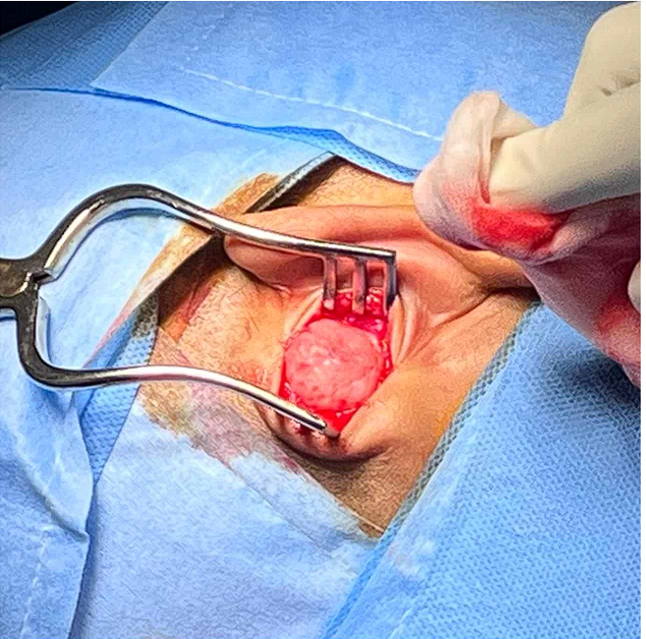
Figure 3. Intraoperative image of osteoma

Figure 4. Intraoperative drilling of the tumour

Figure 5. After complete excision of the tumour
DISCUSSION
Osteomas are benign tumours of mesenchymal origin.1 They are seen most commonly in frontal and ethmoid sinuses. They are seen rarely in the temporal bone. Within temporal bone osteomas are most commonly reported in the external auditory canal, but rarely in the mastoid. Mastoid osteomas have incidence of 0.1-1% of all head and neck benign tumours. Although etiology of mastoid osteomas is still unknown,2 its occurrence can be syndromic or non- syndromic.3 Example for syndromic type include gardener’s syndrome. Osteomas which are of non-syndromic include trauma, inflammation, metaplasia, pituitary dysfunction, chronic infection, surgery, irradiation, and genetics. Osteomas has varied histology including cartilaginous, compact, spongy, mixed.4
Usually osteomas are asymptomatic, solitary, gradually progressive and rarely greater than 3cm size. However, depending on size it can cause facial palsy, sensation of ear fullness, pressure related pain, hearing loss etc.2 Mastoid osteomas have higher incidence in female, predominantly seen in second and third decades of life.2 Differential diagnosis include exostoses, osteoblastic metastasis, osteosarcoma, ossifying fibroma etc. Investigation of choice is CT scan. Radiographically they appear as well-circumscribed osseous growth attached to outer cortex of mastoid bone.2 Asymptomatic patients can be followed up with observation. Treatment is surgical excision for symptomatic and unaesthetic cases. Surgery should include careful removal of periosteum and safe margin of cortex around it. Recurrence is very rare. Malignant transformation has never been reported.
End Note
Author Information
- Dr Sree L, DNB Resident, Department of Otorhinolaryngology, KIMS Health, Trivandrum
- Dr M Suresh Kumar, MS ENT, Senior Consultant, Department of Otorhinolaryngology, KIMS Health, Trivandrum
Conflict of Interest: None declared
REFERENCEs
- Abdel Tawab HM, Kumar V R, Tabook SMS. Osteoma Presenting as a Painless Solitary Mastoid Swelling. Case Reports in Otolaryngology. 2015;2015:1–3.
[Pubmed] | [Crossref] - Borissova IB, Venturin JS, Claro-Woodruff WI, Shintaku WH. Mastoid osteoma: A rare incidental finding in an orthodontic patient. Imaging Sci Dent. 2020 Dec;50(4):347–51.
[Pubmed]| [Crossref] - Kandakure VT, Lahane VJ, Mishra S. Osteoma of Mastoid Bone; A Rare Presentation: Case Report. Indian J Otolaryngol Head Neck Surg. 2019 Nov;71(S2):1030–2.
[Pubmed]| [Crossref] - Al-Yahya SNSH, Wan Hamizan AK, Zainuddin N, Arshad AI, Ismail F. Mastoid osteoma: Report of a rare case. Egyptian Journal of Ear, Nose, Throat and Allied Sciences. 2015 Jul;16(2):189–91.
[Source]