Original Research Published on June 20, 2024
Compliance to Multimodality Management in Locally Advanced Head and Neck Malignancies
Reshmi Francis Vadakkan1, Remya Varghese1, Shibu George2, Bineetha T Thomas3
1. MBBS Student, Govt Medical College, Kottayam; 2. Department of Otorhinolaryngology, Government Medical College, Kottayam;
3. Department of Radiation Oncology, Govt Medical College, Kottayam*
ABSTRACT
Background: Head and Neck cancer is the 8th most common cancer globally and the 3rd most common in India. It includes cancers of the oral cavity, oropharynx, nasopharynx, larynx, hypopharynx, paranasal sinuses, salivary glands and the ear.
Most cases are managed by more than one approach like surgery radiotherapy or chemotherapy. The particularly long regimen of multimodality management may present many factors that affect patient compliance. Attempts at studying such factors can go a long way in ensuring completion of the treatment plan for curative or palliative intent, reducing recurrence and improving quality of life of the patients.
Objectives: To study compliance to multimodality management in locally advanced head & neck malignancies and to determine the association with various factors
Methodology: This is a cross-sectional study to determine the compliance to multimodality management of locally advanced head and neck malignancies. The study subjects were persons diagnosed with locally advanced head and neck malignancies, who have been receiving more than one modality of cancer management which may include surgery, chemotherapy or radiotherapy from our institution between January 2022 to December 2022.The subjects who satisfied the inclusion criteria based on the cancer-patient records were interviewed with a semi structured format via telephone. The significance of all variables was calculated using chi-square analysis
Results: This study determined the overall noncompliance among patients of locally advanced head and neck malignancies to be 20%
The only factor that was found to have a significant association with noncompliance was lack of confidence in the treatment regimen. {P=0.0279}
Conclusion: A statistically significant association was observed between noncompliance and lack of confidence in treatment regimen.
Keywords: Otorhinolaryngology, Head and Neck cancer, Multimodal management, Radiotherapy, Chemotherapy
INTRODUCTION
Most head and neck malignancies are managed by multiple treatment modalities which may include combination of surgery, chemotherapy or radiotherapy in different permutations. The very intricate anatomy and prime functions of the organs involved make it cumbersome to manage Head & Neck malignancy with a single treatment modality.
Radiotherapy: It refers to the use of various types of ionising radiations like from a beam of X rays or subatomic particles. Essentially, Radiotherapy is of two types; teletherapy and brachytherapy. Teletherapy or external beam therapy utilises an external source of radiation. In brachytherapy a naturally occurring radioactive substance placed inside the body.1 Radiotherapy works by disrupting the process of cell division resulting in what is called a mitotic catastrophe.2 Radiotherapy is especially deleterious to cancer cell lines which divide at a much-accelerated rate as compared to normal cells. It is usually administered in multiple sittings spanning a number of weeks. This is called fractionation.
Fractionation is based on the 4 R’s of radiobiology, Repair, Repopulation, Redistribution and Reoxygenation.3 Fractionation allows time for the normal cells to recover from the effects of radiotherapy while cancer cells are permanently damaged. The most commonly prescribed fractionation is about 1.8-2.2 Gy per fraction and five fractions in a week.4 Radiotoxicity refers to the adverse effects that occur following radiotherapy due to damage of normal cells.5
Chemotherapy: It uses drugs to destroy the rapidly proliferating cancer cells. Traditional chemotherapeutic agents may induce delayed results and a hence a combination of agents is often used to produce an adequate response. Chemotherapy may be the primary treatment, administered before surgery (Neoadjuvant), following the surgery (Adjuvant), or concurrent.6 Induction chemotherapy prior to concurrent chemoradiation has shown significant results in early eradication of micro metastasis.7
Surgery: This modality often has a definite curative intent as compared to the often-palliative intent of the other two modalities. However, the complicated anatomy of the head and neck make it a difficult area to manoeuvre. Loss of functionality due to removal of a part or whole of the prime structures is another drawback, Surgical risks prevent it from being adopted in frail and surgically unfit individuals.
METHODOLOGY
A retrospective study was done based on cancer patient records of Government Medical College Kottayam, between January 2022 to December 2022.The study subjects were patients diagnosed with head & neck malignancy in whom a regimen involving any 2 of surgery, chemotherapy or radiotherapy were initiated during this period (irrespective of whether treatment was completed during or after the period). Patients who met their end during the course of treatment were excluded. A sample size of 85 was obtained based on the inclusion & exclusion criteria.
Non-compliance was defined as lack of completion of regimen or a delay of “more than” or “equal to” 1 week in the set appointment dates.
The various factors that were analysed were age, sex, marital status, occupation, address, type of malignancy, AJCC staging, modalities adopted, ration card, financial assistance, confidence, support of family & friends and side effects following treatment.
The subjects were interviewed over telephone and data collected for analysis on a semi-structured proforma.
RESULTS & DISCUSSION
Observations and results of the study are represented in Table 1 and 2.
Out of the 85 subjects an overall compliance of 80% was found. A statistically significant association was found between non-compliance and lack of confidence in treatment regimen (p=0.0279).
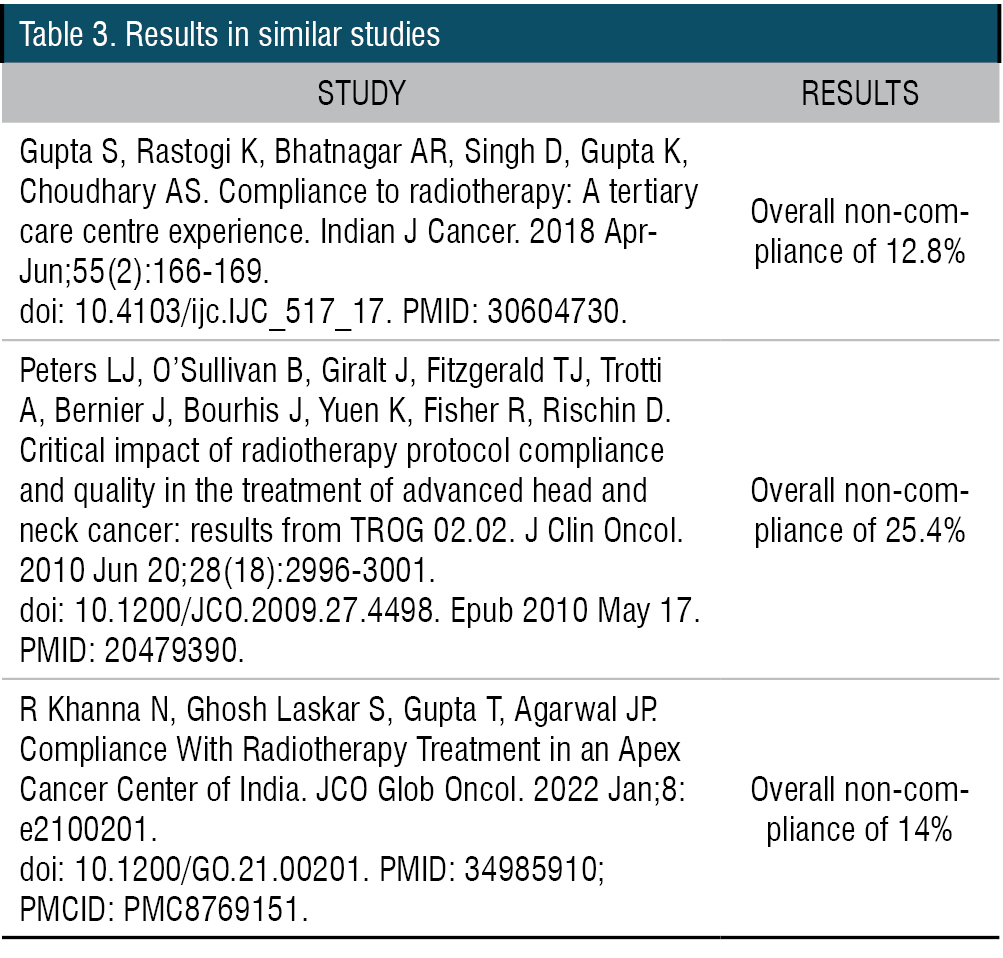
We also reviewed the results in similar studies (Table 3).


CONCLUSIONS
Noncompliance rates are similar to other studies cited in literature.
A statistically significant association was found between non-compliance and lack of confidence in treatment regimen.
RECOMENDATIONS
Psychological counselling may be offered to everyone undergoing multimodality management with follow-up sessions.
The treatment regimen and how it can help the person should be thoroughly explained.
Longer time slots may be allotted to such patients for the doctor to create a better doctor patient relationship and empathize and understand the challenges faced by the patient.
LIMITATIONS OF THE STUDY
The limitations of the study are small sample size, recall bias, non-response bias and the telephonic nature of interview.
End Note
Author Information
- Reshmi Francis Vadakkan, 7th Semester MBBS, Govt Medical College, Kottayam
- Remya Varghese, 7th Semester MBBS, Govt Medical College, Kottayam
- Dr Shibu George, Professor, Department of Otorhinolaryngology, Govt Medical College, Kottayam
- Dr Bineetha T Thomas, Associate Professor, Department of Radiation Oncology, Govt Medical College, Kottayam
Financial support: Nil
Conflict of Interest: None Declared
Editor’s notes: Treatment compliance is crucial in the management of malignancy. This study sheds light to an unexplored aspect of cancer treatment. The effort and interest shown by the main authors who are medical students under the able guidance of their faculty are well appreciated.
REFERENCES
- Maani EV, Maani CV. Radiation Therapy. 2022 Oct 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
[Pubmed] - Maier P, Hartmann L, Wenz F, Herskind C. Cellular Pathways in Response to Ionizing Radiation and Their Targetability for Tumor Radiosensitization. Int J Mol Sci. 2016 Jan 14;17(1):102.
[Pubmed] | [Crossref] - Withers, H.R., 1975. The four R’s of radiotherapy. In Advances in radiation biology (Vol. 5, pp. 241- 271). Elsevier.
[Source] - Gupta S, Rastogi K, Bhatnagar AR, Singh D, Gupta K, Choudhary AS. Compliance to radiotherapy: A tertiary care centre experience. Indian J Cancer. 2018 Apr-Jun;55(2):166-169.
[Pubmed] | [Crossref] - Sroussi HY, Epstein JB, Bensadoun RJ, Saunders DP, Lalla RV, Migliorati CA, Heaivilin N, Zumsteg ZS. Common oral complications of head and neck cancer radiation therapy Cancer Med. 2017 Dec;6(12):2918-2931.
[Pubmed] | [Crossref] - Amjad MT, Chidharla A, Kasi A. Cancer Chemotherapy. [Updated 2023 Feb 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
[Pubmed] - Nazeer F, Poulose JV, Kainickal CT. Induction chemotherapy in nasopharyngeal carcinoma- A systematic review of phase III clinical trials. Cancer Treat Res Commun. 2022; 32:100589.
[Pubmed] | [Crossref]