Original Research Published on June 20, 2024
A Prospective Study on Safety of Bipolar Diathermy in Thyroid Surgery
Prathap R1, Asim PA1, Vivekanand A1, Swathi Krishna1
1. Department of ENT, Karuna Medical College, Palakkad, Kerala*
ABSTRACT
Introduction: Thyroidectomy is one of the commonly performed surgeries with minimal morbidity. With the advent of newer technology the average surgical duration, post operative hospital stay and post operative complication rates has been reduced even more as compared to that a decade ago. This study is aimed to find out the safety profile of use of bipolar cauterisation technique in haemostatic management and the incidence of postoperative complications in thyroidectomy.
Materials and Methods: This is a prospective observational study in a tertiary care hospital. A total of 51 patients in the age group 18-80 years who underwent thyroidectomy surgery between 2021 January to June 2022 is evaluated and the results were analysed.
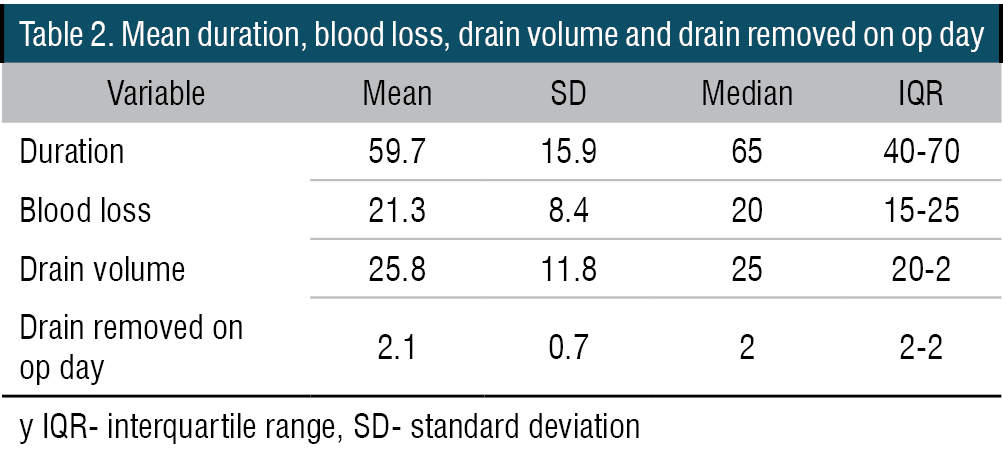
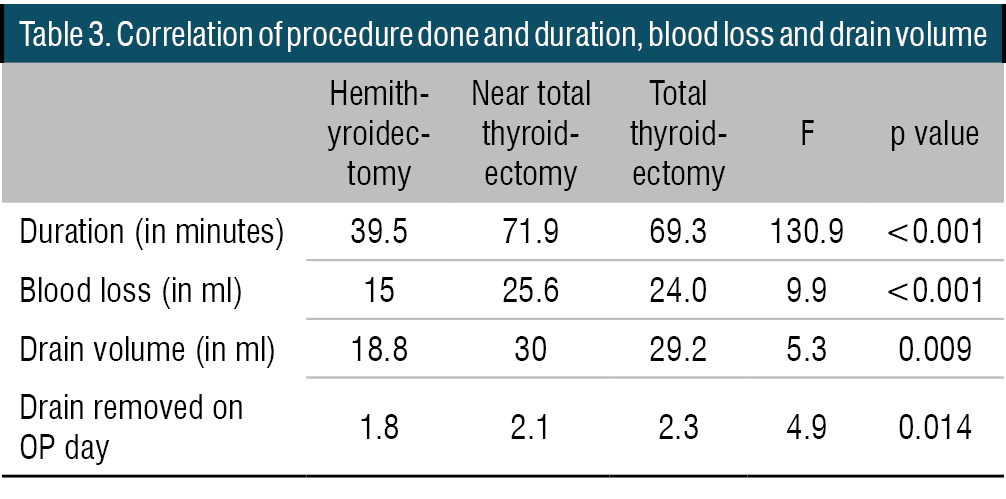
Results: Out of the 51 patients we performed 26 total, 8 near total thyroidectomy and 17 hemithyroidectomy. The average surgical duration for hemithyroidectomy was 39.5 minutes and that of total thyroidectomy was 69.3 minutes. Average blood loss during the surgery was 15 ml and 24 ml in hemithyroidectomy and total thyroidectomy groups respectively. The average post operative surgical drain volume was 18.3 ml in the hemithyroidectomy group and in near total and total thyroidectomy group it was close to 30 ml. The drain was able to be removed in most of the patients by day two. No statistically significant difference were found between the duration of procedure and post operative complication.
Conclusion: The use of bipolar thermal device provide a cost-effective method in achieving haemostasis of the thyroid pedicle. This is a promising alternative to standard ligature techniques. It offers reduced operative time there by reducing peri and post operative morbidity and mortality.
Keywords: Bipolar Cautery, Thyroidectomy
Introduction
The incidence of thyroid related diseases is very common in general population worldwide. A handful of disorders of this endocrine gland can be managed with pharmaceutical agents, but majority of the disorders usually indicate the need for surgery. The origin of thyroid surgery date back to 12-13th century and was associated with high rate of post operative morbidity and mortality. Due to these troublesome challenges the surgery of thyroid gland became less popular during 17-18th century. The thyroid surgeries become widely accepted after Theodor Kocher’s works in this field and he is considered as the father of thyroid surgeries.1
At present thyroidectomy is a common surgical procedure, usually performed by ENT surgeons, general surgeons or oncosurgeons. The safety profile of the procedure has dramatically improved when compared with the olden period. This reduction in the intraoperative and postoperative adverse events can be attributed to the developments that lead to proper technique, operative instruments as well as modern technology assisted devices in surgical arena.
The intra operative haemorrhage during thyroid surgeries were managed using standard ligature techniques, but with the invention of biomedical devices such as bipolar cauterisation, ligature clips and harmonic scalpel, the average surgical duration, post operative hospital stay and post operative complication rates has been reduced even more as compared to that a decade ago.
Bipolar cauterisation is an easily available, cost-effective electrocautery device to control bleeding events during surgery. When compared to monopolar cautery device, the bipolar machine causes less damage to the adjacent tissues. This is of an added advantage when doing thyroidectomies, thereby help to avoid or causing greater damage to recurrent laryngeal nerve and parathyroids while manipulating thyroid pedicle. The proximity of Recurrent laryngeal nerve (RLN) to the thyroid inferior pedicle often causes difficulty in managing the inferior pole bleeding. The use of bipolar device is a safe option and is considered as an alternative to standard pedicle ligation and in capsular dissection also.2,3
Though considered as a safe technique, this study is aimed to find out the safety profile of use of bipolar cauterisation technique in haemostatic management of thyroid pedicle by evaluating the surgical procedure duration, post operative suction drain volume, number of days with drain in situ, average hospital stay, post operative complications incidence of recurrent laryngeal nerve paresis or palsy and hypocalcaemia symptoms.
METHODS
Our study was a prospective observational study among thyroidectomy patients during the time period 2021 January to June 2022 at a tertiary care centre in Palakkad district Kerala.
All patients of the age group 18-80 years who had undergone any type of thyroidectomy and who were willing for participation in the clinical study were included. Patient who had undergone completion thyroidectomy following a previous hemithyroidectomy were excluded from the study.
SURGICAL TECHNIQUE
A standard Kocher’s neck incision was put in most of the cases, in some exceptional cases a transverse neck incision was put based on the tumour size. Sub platysmal skin flap raised superiorly and inferiorly. Investing layer of cervical fascia over strap muscles divided in the midline and strap muscles retracted laterally. Joule’s forceps placed. Middle thyroid vein identified and cauterised using bipolar electrocautery close to the glandular surface. The superior and inferior pedicle identified and electrocauterized close to the gland to avoid injury to external branch of superior and recurrent laryngeal nerve respectively (Figures 1 and 2). The thyroid gland made free from its bed and capsular attachment by meticulous dissection. Thyroid gland removed using bipolar cautery dissection. Haemostasis achieved. We usually keep a small gel foam piece soaked in lignocaine on the para tracheal space following thyroidectomy. Suction drain kept and fixed using 2-0 or 1-0 silk sutures. Strap muscles approximated using 3-0 vicryl, sub platysmal suturing using the same material. Skin closure by 3-0 ethilon or surgical staplers.
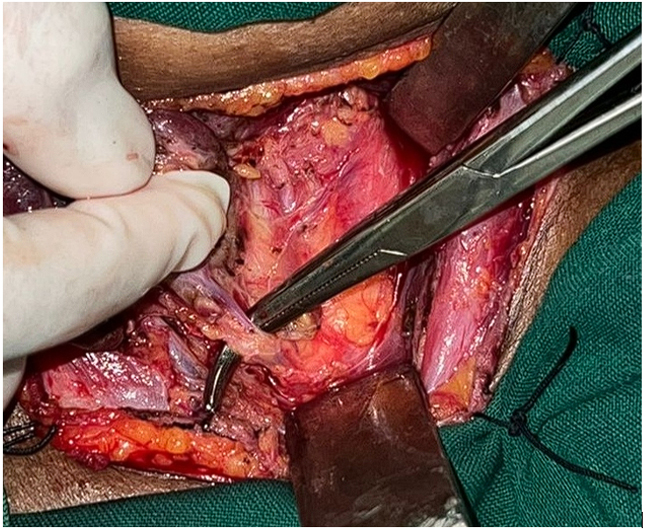
Figure 1. Showing dissection of thyroid vascular pedicle
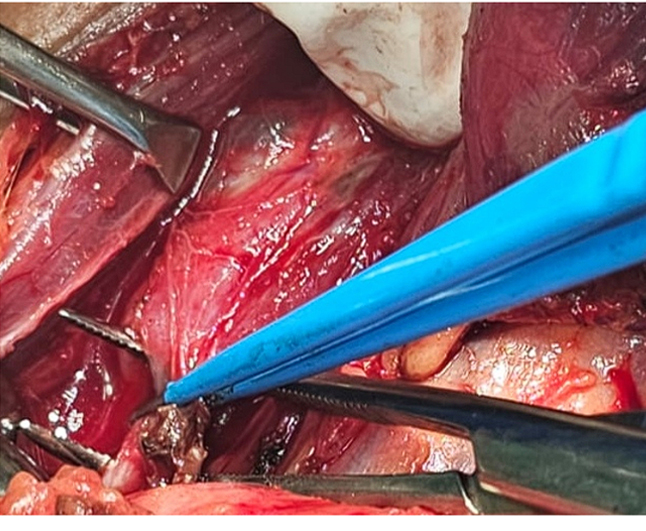
Figure 2. Showing use of bipolar cautery in achieving hemostasis of vascular pedicle
In our study the surgical procedure duration was calculated from the time of incision to complete skin closure.
Post operatively on Day 1 we routinely checked for Haemoglobin and PCV values and started on tablet thyronorm 1.6-1.8 mg/kg for total thyroidectomy patients. On day 2 we calculated corrected calcium levels, and administered required calcium replacement if necessary, and patient will be discharged usually on day 2 or day 3. Suture / stapler removal on post-operative day 7, and on post-operative day 30 thyroid function tests will be repeated and dose titrated accordingly.
Patients were examined for signs and symptoms of hypocalcaemia on day of discharge and were also subjected for a videolaryngoscopic examination to know the status of vocal fold paresis or palsy.
RESULTS AND ANALYSIS
51 patients were included the study, of which three were males and 48 out of 51 were females. Majority of the patients belonged in the age group of 31-50 years ( 56.9 percentage). The age distribution of the study population is shown in table 1. Multinodular goitre was the most common condition that we addressed (29 out of 51) (Figure 3). We performed 26 total thyroidectomy and 8 near total thyroidectomy during the study period. The average surgical duration for hemithyroidectomy was 39.5 minutes and that of total thyroidectomy was 69.3 minutes. Average blood loss during the surgery was 15 ml and 24 ml in hemithyroidectomy and total thyroidectomy groups respectively. The average post operative surgical drain volume was 18.3 ml in the hemithyroidectomy group and in near total and total thyroidectomy group it was close to 30 ml. The drain was able to be removed in most of the patients by day two. On doing ANOVA test the duration of procedure, amount of blood loss and drain removed showed statistically significant when compared among the type of surgery performed (Tables 2, 3, 4 and 5).
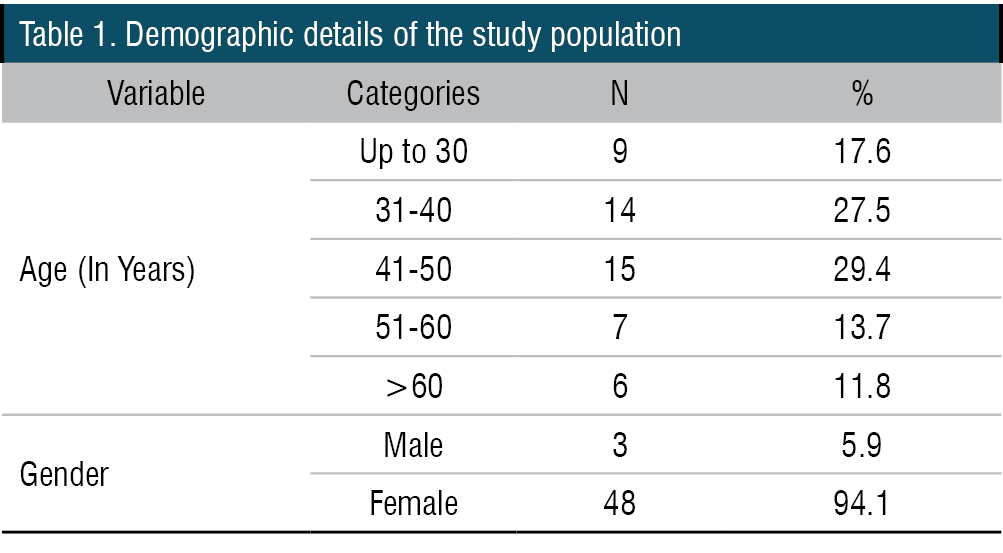
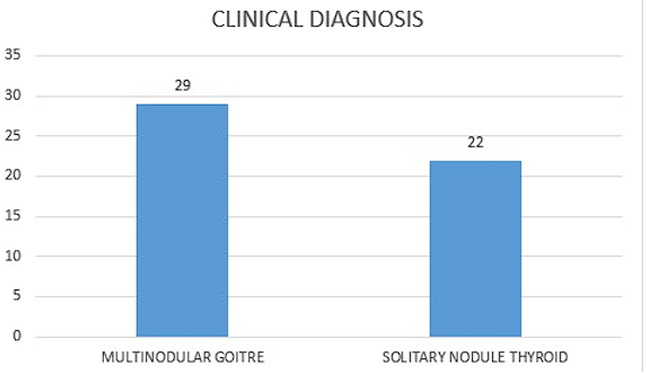
Figure 3. Graph showing distribution of preoperative disease condition

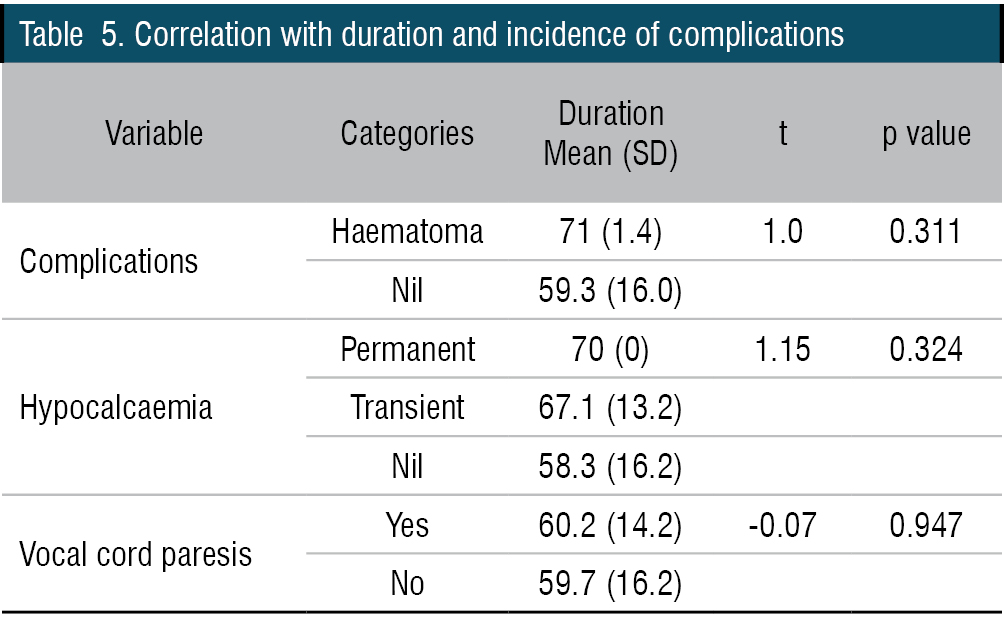
The surgery was uneventful in most of the patients, two total thyroidectomy patients had haematoma formation in the post operative period. Seven patients had transient hypocalcaemia symptoms and one had permanent hypocalcaemia. The incidence of vocal cord paresis was less than 10 percent in our study and most of the patients with vocal fold involvement were in the total thyroidectomy group. We couldn’t find any statistically significant correlation between the duration of procedure and post operative complications.
DISCUSSION
Thyroidectomy, of any type often found to be challenging even in the hands of experienced head and neck surgeons. One of the major factors making the surgery troublesome is the complex anatomy of the neck. Among the various difficulties faced intra operatively, the primary haemorrhage is found to be the important one.4 The ligature of the vascular pedicles of the thyroid gland is one of the crucial steps. At times this can be time consuming also, there by significantly increasing the duration of the procedure. The close proximity of the superior and recurrent laryngeal nerves to the pedicle make the process of achieving haemostasis even more tricky. Any kind of damage to these nerves either neuropraxia due to traction or nerve fibre damage, will affect the physiology of voice production in the post operative period. This can cause functional as well as psychological concerns to the patients. An improper haemostatic control during surgery may even lead to hematoma formation in the immediate post op period, which further increasing the hospital stay duration.5
To achieve haemostasis, the traditional techniques include use of standard ligatures, sutures, or ligature clips. In recent years the use of thermal devices has gained attention as an alternative method in achieving pedicle haemostasis. One among the thermal devices is a more popular equipment unit in most of the surgical departments is bipolar electrocautery. This device helps in achieving haemostasis by generating heat and sealing the tissue while passing the electric current. Though monopolar cautery uses the same mechanism, the bipolar devices coagulate the tissues in a very small area, there by reducing the damage to adjacent tissues.2
The efficacy and safety of this technique has been investigated and found to be an effective method in controlling haemostasis intraoperatively. The advantages include faster technique there by significantly reducing the duration of the procedure, and less risk of post operative complications. Similar advantages were found in our study also, as the duration of hemithyroidectomy was close to half an hour and for total it was little more than an hour. Another advantage of bipolar cautery is that it avoids the need for knots or clips. The slippage of these standard ligature is found to be a cause for post operative hematoma formation. The knots or clips also found to have certain role in suture related complication also.
In a study conducted by Balghari KW et al, where they evaluated the safety of bipolar cautery device in relation to RLN injury during thyroidectomies, none of the patients developed any vocal cord palsy or weakness (n=52). In our study 5 patients had weakness of the vocal cord post surgically.6 In a similar study conducted by Jawad et al, comparing the use of ligasure and bipolar device in total and hemithyroidectomy, the results showed no statistical difference between these two devices in terms of incidence of post operative complications. This study emphasizes the use of bipolar device as a cost-effective tool in achieving haemostasis.7
Best AE et al, concluded with their study that, using alternative sources of cautery compared with traditional techniques significantly reduced post operative hematoma incidence. Interestingly their study concluded that use of these energy devices increased the operative time by 4.95 minutes. This may be due to the inexperience of the surgeon in performing cauterisation of the pedicle or time taken to set up the cautery unit.8 Hegab AM compared the use of bipolar with standard ligature in total thyroidectomy cases. The mean difference in operative time duration was 21 minutes and mean difference in blood loss was 20ml. the results showed statistically significance in terms of post operative pain also.9
Prakash Om et al also concluded that bipolar cauterization significantly reduced the surgery time, duration of hospital stay and post operative complication rates when compared with traditional suture ligature.10 Similar results were found in a study conducted by Vasuki R et al.11
Kim WW et al compared the use of ultrasonic advanced bipolar device and bipolar device during thyroid surgeries and found that both are equally effective in reducing post operative complications.12 A Study by Challa S et al concluded that bipolar unit is a better method for haemostatic control than ligasure and harmonic scalpel in terms of cost of the devices.13
Transient hypocalcaemia was noted in 7 out of 51 patients in our study. All these patients were weaned off calcium supplements later. The development of this hypocalcaemia can be because of damaging the principle vascular system to the parathyroid gland intraoperatively. Only one case of permanent hypoparathyroidism was found in our study.
Vocal cord paresis was found in 5 patients in our study and no cases of vocal cord palsy was noted. The vocal cord paresis may be because of the thermal injury leading to neuropraxia of the laryngeal nerves and because of difficulty in finding plane of dissection due to tissue adhesions. This highlights the need for avoiding thermal damage while using high energy devices. We authors advice meticulous dissection of pedicle, use of saline irrigation and less contact time of the bipolar cautery to avoid heat related injury to the adjacent vital structures.
Though the proponents of this technique advocate the wide use of bipolar cautery, the concerns raised regarding the potential thermal injury to the nearby anatomical structures cannot be neglected. Further studies are of the need at present to fully establish the safety and efficacy of this technique.
Authors here by conclude that, use of bipolar thermal device provide a cost-effective method in achieving haemostasis of the thyroid pedicle. This is a promising alternative to standard ligature techniques. It offers reduced operative time there by reducing peri and post operative morbidity and mortality. Skilled technique, surgeon expertise, adequate and proper training are of paramount importance in ensuring better outcomes and to avoiding inadvertent thermal tissue damage.
End Note
Author Information
- Dr. Prathap R, DNB ENT, Associate Professor, Department of ENT, Karuna Medical College, Palakkad, Kerala.
- Dr. Asim PA, MS ENT, Associate Professor, Department of ENT, Karuna Medical College, Palakkad, Kerala.
- Dr. Vivekanand A, MS ENT, Assistant Professor, Department of ENT, Karuna Medical College, Palakkad, Kerala.
- Dr. Swathi Krishna, MS ENT, Assistant Professor, Department of ENT, Karuna Medical College, Palakkad, Kerala.
Acknowledgements: The authors would like to express our gratitude to Dr Jeby Jose, who helped us with compilation of data and statistical analysis.
Financial support: Nil
Ethical Standards: The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and our institutional guidelines on human experimentation and with the Helsinki declaration of 1975, as revised in 2008.
REFERENCES
- Ludwig B, Ludwig M, Dziekiewicz A, Mikula A, Ciesk J, Biernet S et al. Modern surgical techniques of thyroidectomy and advances in the prevention and treatment of peroperative complications. Cancers. 2023;15(11):2931.
[Pubmed] | [Crossref] - Smith RB, Coughlin A. Thyroidectomy hemostasis. Otolaryngol Clin N Am. 2016;49(3):727-748.
[Pubmed] | [Crossref] - Lee E, Tong JY, Pasick LJ, Benito DA, Joshi A, Thakkar PG et al. complications associated with energy-based devices during thyroidectomy from 2010-2020. World J Otorhinolaryngol Head Neck Surg. 2023;9:35-44.
[Crossref] - Zhang X, Du W, Fang Q. Risk factors for postoperative haemorrhage after total thyroidectomy: clinical results based on 2678 patients. Sci Rep.2017;7:7075.
[Pubmed] | [Crossref] - Edafe O, Balasubramanian SP. Reoperation for bleeding after thyroid and parathyroid surgery: Incidence, Risk factors, Prevention and Management. World J Surg. 2020;44:1156-1162.
[Pubmed] | [Crossref] - Balghari KW, Abbas N, Khan MA, Ilyas M, Islam MU, Ijaz MT. Assessment of safety of bipolar diathermy regarding recurrent laryngeal nerve damage in thyroid surgery. Pak Postgrad Med J. 2020;30(02):271.
[Crossref] - Jawad NK, Al-Harbawi LQ, Ullawerdi KS. Compare using of ligasure and conventional bipolar device in total thyroidectomy. Retrospective study. Teikyo Med J. 2021;44(06):2955-2960.
[Source] - Best CAE, Quimby AE. Alternative sources of cautery may improve post operative hematoma rates but increase operative time in thyroid surgery. Sci Rep.2021;11:22569.
[Source] - Hegab AM. Comparative study between bipolar electro cautery and knot tying technique in total thyroidectomy. AIMJ. 2021;9:7-11.
[Crossref] - Prakash O, Chandrasekhar S, Mathews J, George R, Suprej K, Mathew J et al. Bipolar cautery versus conventional suture ligation of vascular pedicles in thyroidectomy: a comparative clinical study. Int Surg J. 2021;8:1181-1184.
[Crossref] - Vasuki R, Thanmaran NB, Malathi V, Kujur L. A study of use of bipolar cautery in thyroidectomy. Int Surg J. 2017;4:1059-1064.
[Crossref] - Kim WW, Cho J, Jeon YS et al. Prospective, randomized , comparative , multicenter study of the hybrid ultrasonic advanced bipolar device and the ultrasonic coagulating shears in open thyroidectomy. Surgical Innovation. 2021;28(1):41-47.
[Crossref] - Challa S, Surapaneni S. Suture less thyroidectomy vascular control using bipolar electrothermal cautery. J Evol Med Dent Sci. 2012;1(6):1083-1086.