Case Report Published on December 20, 2023
Nasolacrimal Duct Primary B Cell Lymphoma -
A Case Report
Paul Samuel1, Rachel Benny2
1. Department of ENT, Cosmopolitan Hospital, Trivandrum, Kerala;
2. Department of Ophthalmology, Chaithanya Eye Hospital and Research Institute, Thiruvananthapuram, Kerala*
ABSTRACT
Non-hodgkin lymphoma (NHL) is a type of haematological malignancy originating from lymphocytes. NHL in nasal cavity and sinuses are rare findings. This case report highlights the importance of proper clinical history and examination along with management protocols to avoid missing a rare, but deadly disease.
A middle aged lady presented to our out-patient wing with left sided epiphora for one year. Initial imaging showed findings favourable to diagnosis of mucocele obstructing the nasolacrimal duct outflow. However, a biopsy with immunohistopathological study from the lesion demonstrated a diffuse large B cell lymphoma.
Keywords: Primary Neoplasm, Primary Diffuse B Cell Lymphoma, B Cell Lymphoma, Naso-Lacrimal Duct Obstruction, Lacrimal Sac Tumours
Introduction
Nasolacrimal duct (NLD) obstruction may be congenital or acquired. Acquired causes of nasolacrimal duct obstruction could be primary or secondary. There are many causes for secondary acquired nasolacrimal duct obstruction; however the most common causes are infectious, inflammatory, neoplastic, traumatic and mechanical. Neoplastic cause of nasolacrimal duct obstruction can be due to primary tumours of lacrimal system (papillomas, lymphomas, squamous cell carcinomas and melanomas). Nasolacrimal duct obstruction can also be caused by tumours in adjacent tissues, such as basal cell carcinomas, squamous cell carcinomas, adenoid cystic carcinomas, leukaemia and lymphomas. Secondary acquired nasolacrimal duct can also be rarely caused by metastases from breast carcinoma, malignant melanoma or prostate carcinomas.
Lymphoma is the second most common primary neoplasm occurring in head and neck. Non-Hodgkin’s lymphoma (NHL) is a group of neoplasms that originate from cells of lympho-reticular system. Nasal cavity and PNS are rarely affected by primary NHL. Large B cell lymphoma (LBCL) is the most common NHL, and is a fast growing malignancy that arises inside or outside of the lymphatic system.
Tumours of lacrimal drainage system are rare. Malignant lymphomas account for 6% of all lacrimal sac tumours. They are mostly secondary to systemic lymphoreticular malignancies. Primary NHL of lacrimal sac is extremely rare. Its symptoms are usually non-specific and thus easy to misdiagnose. We report a primary diffuse B cell lymphoma involving lateral wall of left inferior nasal meatus, nasolacrimal duct and left lacrimal sac, which was initially misdiagnosed as a mucocele.
Case Report
A 42 year old lady presented to the out-patient department (OPD) with a history of left sided epiphora since 1 year and a mass around her left lacrimal sac (Figure 1&2) for which she consulted another tertiary ophthalmology centre a year back, where she was treated with ofloxacin eye drops and she was lost to follow up. She presented herself with a CT report of PNS which showed mildly hyperdense minimally enhancing soft tissue measuring 19x15x19 mm in the left inferior meatus, blocking the exit of NLD and extending superiorly widening the nasolacrimal duct. Superior part of the lesion in the lacrimal sac region measured 17x13x15cmm (Figure 3, 4 & 5).

Figure 1. Left sided lacrimal area swelling

Figure 2. Left sided lacrimal area swelling (side view)
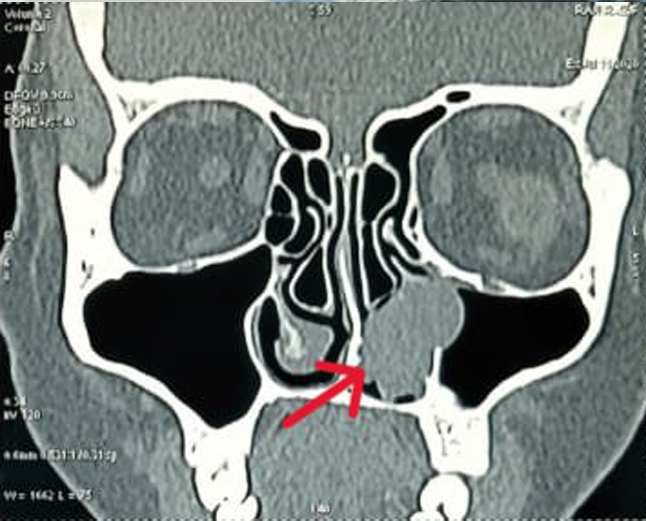
Figure 3. CT scan Paranasal sinus coronal view showing the mass in the inferior meatus

Figure 4. CT scan Paranasal sinus Coronal view showing the mass in the lacrimal sac region
On examination there was a firm swelling in the left lacrimal sac region slightly extending into orbit, also the sac cannot be emptied on pressure. Diagnostic endoscopy showed a fleshy mass in the inferior meatus (Figure 6). We conducted an endoscopy guided excision biopsy of the inferior meatal mass in order to confirm the diagnosis. Specimen was sent for histopathological examination.
Immunohistopathological examination done on the excision biopsy sample revealed positive for CD20, CD10, BCL6, BCL2, MUM1 in 76-100% of lesional cells, and KI-67 positivity in 51-75% lesional cells. Based on the immunohistopathological appearance, she was concluded to have primary diffuse B cell lymphoma (DBCL)- germinal centre type.
She was subsequently referred to the Regional Cancer Centre (RCC), Trivandrum for further oncological evaluations and treatment. She underwent 6 cycles of chemotherapy with standard R- CHOP regimen and involved field radiotherapy. After completion of the R-CHOP, the epiphora and the palpable mass on the left medial canthus had resolved .She has since been on regular follow-up.

Figure 5. CT scan Paranasal sinus axial view showing the mass in the inferior meatus and widening of nasolacrimal duct
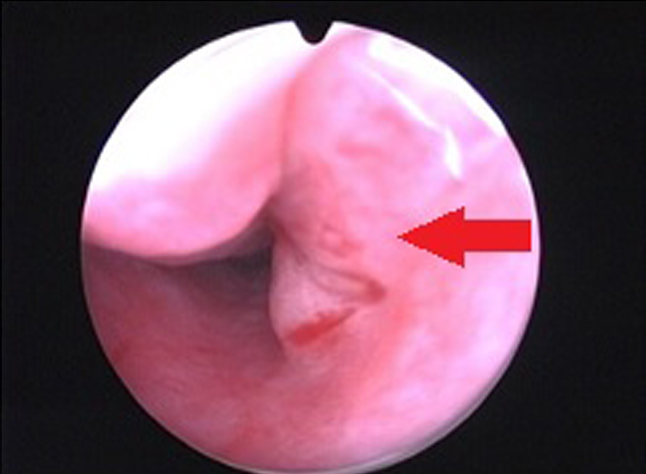
Figure 6. Endoscopic views of the mass in the left inferior meatus
Discussion
Primary lymphoid tumours of nasal cavity and lacrimal sac are encountered rarely in clinical practice. Among lacrimal sac tumours, 55% of the reported were considered malignant among which 71% where of epithelial origin. Malignant lymphomas accounted for 6% of all lacrimal sac tumours.1,2 Primary lacrimal sac lymphomas usually occur in elderly people. Previous studies demonstrated that 5 year survival rate between 20% and 65%3 and much poorer prognosis for patients with diffuse B cell lymphoma (DBCL) involving the ocular adnexal region. Mostly symptoms are nonspecific and get misdiagnosed as dacrocystitis.
In case of malignant lacrimal sac tumours correct diagnosis occurs only in <15%. Some patients get diagnosed inadvertently during dacrocystorhinostomy or other procedures. Biopsy must be taken examined to confirm the diagnosis. CT and MRI can aid in arriving at a diagnosis, staging and planning treatment. Discrimination between a mucocele and lymphoma requires pathological tests for confirmation, in addition to imaging.
Systemic chemotherapy is effective in treating localized DLBCL4. The introduction of the R-CHOP regimen has improved the survival rate in DLBCL. Rituximab, a monoclonal chimeric anti- CD20 antibody has been extensively used in treatment of B cell NHL. In combination with chemotherapy has a significant benefit compared to chemotherapy alone in terms of response rate, progression free survival and overall survival in patients with DLBCL.
Conclusion
Primary diffuse large B cell lymphoma involving the nasal cavity and the lacrimal sac is a rare presentation, and is often misdiagnosed as dacryocystitis or mucocele. Prompt diagnosis using imaging techniques and biopsy of the lesion is essential in making an accurate diagnosis.
End Note
Author Information
- Dr. Paul Samuel
Senior Consultant in ENT
Department of ENT, Cosmopolitan Hospital, Trivandrum, Kerala - Dr. Rachel Benny
Junior Resident
Department of Ophthalmology,
Chaithanya Eye Hospital and Research Institute, Thiruvananthapuram, Kerala
Conflict of Interest: None to declare
References
1. Montalban A, Liétin B, Louvrier C, Russier M, Kemeny JL, Mom T, et al. Malignant lacrimal sac tumors. Eur Ann Otorhinolaryngol Head Neck Dis. 2010 Nov;127(5):165–72.
[Pubmed] | [Crossref]
2. Alkatan HM, Al-Harkan DH, Al-Mutlaq M, Maktabi A, Elkhamary SM. Epithelial lacrimal gland tumors: A comprehensive clinicopathologic review of 26 lesions with radiologic correlation. Saudi J Ophthalmol. 2014 Jan;28(1):49–57.
[Pubmed]| [Crossref]
3. Tsao WS, Huang TL, Hsu YH, Chen N, Tsai RK. Primary diffuse large B cell lymphoma of the lacrimal sac. Taiwan J Ophthalmol. 2016 Mar;6(1):42–4.
[Pubmed] | [Crossref]
4. Kakutani S, Takahashi Y, Valencia MaRP, Kakizaki H. Diffuse Large B-Cell Lymphoma of the Lacrimal Sac in a Japanese Patient. Case Rep Ophthalmol. 2019 Jan 3;9(3):516–9.
[Pubmed] | [Crossref]