Original Reasearch Published on December 20, 2023
Effectiveness of Pulse Steroid Therapy in Idiopathic Sudden Sensorineural Hearing Loss- A Prospective Study
Ihsan A T1, Vishnupriya Padmakumar1, Prathibha Ajayakumar1
1. Department of ENT, Jubilee Mission Medical College and Research Institute, Thrissur*
ABSTRACT
Objective: To study the role of initial high dose of intravenous steroids in patients with idiopathic sudden sensorineural hearing loss
Study Design: We did a prospective study of a case series of 20 patients who presented to the Department of Otorhinolaryngology, Jubilee Mission Medical College, with idiopathic sudden sensorineural hearing loss. All patients were put on the same treatment protocol of initial high dose steroids.
Results: Of the 20 patients, 5 cases showed complete recovery, 10 cases showed slight improvement and 4 cases showed no improvement (As per Siegel’s criteria).1 patient was lost to follow up. Mean improvement in hearing was found to be 19.663. No differences were noted in cases of different age, sex, and those with tinnitus and vertigo.
Conclusion: For sudden sensorineural hearing loss the treatment is initial steroid therapy (as per AAO-HNS guidelines 2019). But the exact dose or route of administration of steroid is not mentioned. Our treatment protocol of initial pulse steroid therapy produced a recovery rate, which exceeds the spontaneous recovery rate. In addition, vertigo or tinnitus did not indicate a poor prognosis.
Significance: Initial high dose IV steroid treatment may play a role in the improved recovery rates.
Keywords: Idiopathic Sudden Sensorineural Hearing Loss, Pulse Steroid Therapy
Introduction
Sudden sensorineural hearing loss (SSNHL) is most often defined as sensorineural hearing loss of 30dB or greater over at least three contiguous audiometric frequencies occurring over 72 hours. The majority of patients with sudden SNHL have no identifiable cause for hearing loss and are classified as “idiopathic”. Despite extensive research, controversy remains in the etiology and appropriate care of patients with idiopathic SSNHL.
Regardless of etiology, recovery of hearing thresholds following SSNHL may not occur, may be partial, or can be complete. Factors impacting hearing recovery include age at onset of hearing loss, hearing loss severity and frequencies affected, presence of vertigo, and time between onset of hearing loss and visit with the treating physician.
Tinnitus is usually present. Vertigo is frequent, either spontaneous (as in acute vestibular neuronitis) or as isolated positional vertigo. Sixty-five percent of patients recover completely with or without treatment, most within 2 weeks. Low-frequency losses have a better prognosis than high-frequency losses.
This study follows the course of 20 patients who presented to the department of Otorhinolaryngology of Jubilee Mission Medical College, Thrissur with idiopathic sudden sensorineural hearing loss. All patients were managed with pulse steroid therapy.
Materials and Methods
Study Design: Prospective study
Study Setting: The study was carried out among patients presenting with Idiopathic Sudden Sensorineural hearing Loss to the Department of ENT of Jubilee Mission Medical College and Research institute.
Study period: 12 months (August 2022 to July 2023)
Sample size: We studied all the patients who presented to the ENT OPD with idiopathic sudden sensorineural hearing loss over a period of 1 year (August 2022 to July 2023)- 20 patients
Inclusion criteria: All patients presenting to ENT OPD with complaints of sudden sensorineural hearing loss and underlying cause is not known and presenting within 3 weeks of onset of symptom. All patients with a sensorineural hearing loss of 30dB or greater over at least three contiguous audiometric frequencies occurring over 72 hours
Exclusion criteria: Patients with Mixed or Conductive hearing loss, Age <18 years and >70 years, Preexisting ear disease, Benign and Malignant tumours of ear including acoustic neuroma, glomus jugulare
Methods of Data collection: All patients who presented to the ENT OPD of Jubilee Mission Medical College & Research Institute with sudden onset of sensorineural hearing loss without any identifiable cause
They were be given 1gm IV of methyl prednisolone on the first three days followed by oral steroids (prednisolone/ methyl prednisolone- 1mg/kg dose in tapering dose) and their audiograms were repeated 1 week and 1 month after the treatment to look for any improvement in hearing
Hearing improvement after high dose IV steroids on idiopathic sudden sensorineural hearing loss was assessed using the following criteria:
Siegel’s criteria
Complete recovery: > 30 dB hearing gain / final hearing better than 25 dB
Partial recovery: > 15dB hearing gain and final hearing between 25 dB and 45 dB
Slight improvement: > 15 dB hearing gain and final hearing poorer than 45 dB
No improvement: <15 dB hearing gain
Effectiveness of steroid use was assessed by calculating the hearing gain (Post treatment- Pre treatment PTA). Statistical tests will be done using paired t test and chi square test. SPSS (version 24) software was used for analysis
Results
We studied 20 patients with idiopathic sudden sensorineural hearing loss who presented to the Department of ENT of Jubilee Mission Medical College, Thrissur. Of the 20 patients, 10 were females. The youngest patient in our study was of 20 years old and the oldest patient 73 years old. 15 patients had unilateral hearing loss and 5 patients had bilateral hearing loss. Of the 20 patients included in the study, 9 (45%) had true vertigo (Figure 1) associated with the hearing loss, and 11 (55%) patient had associated tinnitus (Figure 2).
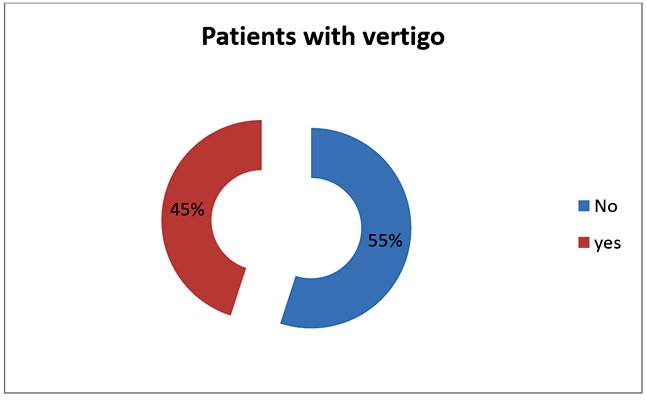
Figure 1. Patients with vertigo
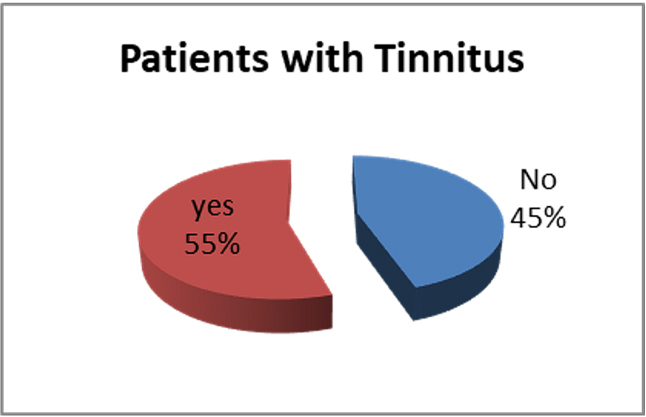
Figure 2. Patients with tinnitus
10 (50%) of the patients presented with profound sensorineural hearing loss, 2 (10%) cases with severe sensorineural hearing loss, 4 (20%) cases of moderately severe hearing loss, 3 (15%) cases of moderate sensorineural hearing loss and 1 (5%) case of mild sensorineural hearing loss (Figure 3)
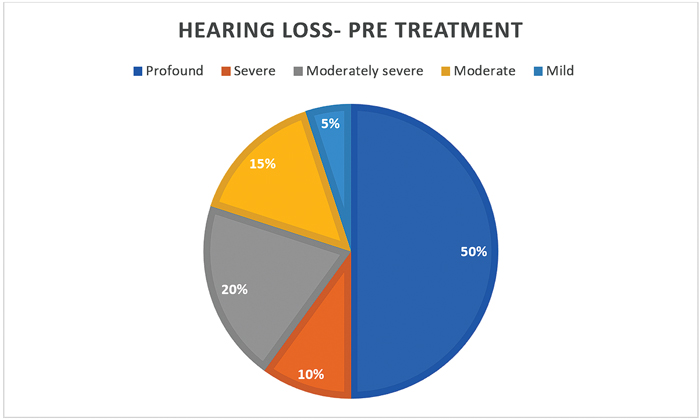
Figure 3. Hearing loss- Pre treatment
Initial IV pulse steroid therapy were given to all the patients for three days followed by tapering doses of oral steroids. PTA was taken post treatment to look for any improvement in hearing. 15 patients showed improvement and 4 patients showed no improvement in hearing.1 patient was lost to follow up. The improvement of hearing was statistically confirmed by applying the paired t test. Mean improvement in hearing was found to be 19.663. Paired samples t test was done – showed that there is significant difference between pre and post PTA (p value <0.0001). This shows that steroids has a major role on treatment of ISSNHL.
Based on Siegel’s Criteria : 5 cases showed complete recovery. 10 cases showed slight improvement. 4 cases showed no improvement (Figure 4).
More than 30 dB hearing gain was seen in 3 patients (15%), > 15 dB hearing gain in 11 patients ( 55 %) and < 15 dB heaing gain was seen in 5 patients ( 25%). 1 patient was lost to follow up (Figure 5). The comparison between pre and post treatment PTA findings are shown in Figure 6.

Figure 4. Improvement based on Siegel’s criteria
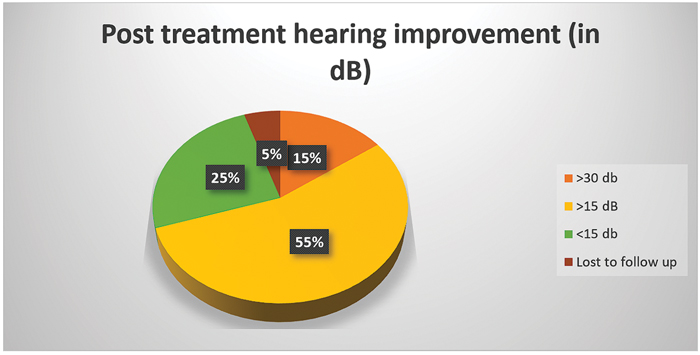
Figure 5. Post treatment hearing improvement (in dB)
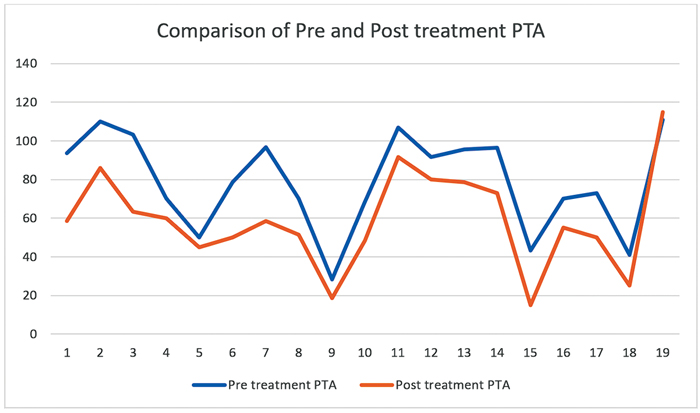
Figure 6. Comparison of pre and post treatment PTA
Mean improvement in hearing was found to be 19.663. Paired samples t test was done – showed that there is significant difference between pre and post PTA (p value <0.0001). This shows that steroids has a major role on treatment of ISSNHL (Table 1)

Discussion
Idiopathic sudden sensorineural hearing loss is defined as a loss of more than 30 dB over three contiguous frequencies occurring in less than 3 days. No identifiable cause is seen in majority of the cases.
Sudden sensorineural hearing loss could, perhaps, be more accurately described as a clinical syndrome, for which there is no identifiable cause in all cases.1 Among the proposed causes of this condition are viral infections and resultant inflammation,2 breaks in Reissner’s membrane causing persistent depolarization of hair cells due to disruption of appropriate ion gradient3, and vascular insult to cochlea.4
Incidence of sudden sensorineural hearing loss was believed to range from 5 – 20 per 100000 population,5 but a recent study suggested a much-increased incidence of up to 160 per 100000 population.6
Most of the patients do not seek advice immediately at the onset of symptom and typical presentation is generally delayed by 48–96 hours.7 We studied 20 patients (between the age group of 20- 73 years) of which one patient was lost to follow up. Of this only 8 patients presented to the hospital within 72 hours.
10 (50%) of the patients presented with profound sensorineural hearing loss, 2 (10%) cases with severe sensorineural hearing loss, 4 (20%) cases of moderately severe hearing loss, 3 (15%) cases of moderate sensorineural hearing loss and 1 (5%) case of mild sensorineural hearing loss in our study.
11 patients (55%) in our study had associated tinnitus. 9 patients (45%) had vertigo associated with hearing loss. Few studies show that presence of associated symptoms like tinnitus and vertigo could result in a poor prognosis in hearing improvement. Our study showed that factors like the presence of vertigo or tinnitus do not seem to affect prognosis.
Although various treatment protocols have been tried, recovery rates of patients with mild, moderate and severe hearing loss still remain 70%, 30%, 10%, respectively, showing remarkable difference according to degree of initial hearing loss.8,9
Despite the results of previous analyses questioning the efficacy of steroids for the treatment of sudden sensorineural hearing loss, this treatment strategy remains the most widely used treatment in various parts of the world.10 Intratympanic steroid injection is an effective salvage option for sudden sensorineural hearing loss with mild and low frequency hearing loss associated with higher remission rates.11 Intratympanic methylprednisolone injections are an effective second line therapy for sudden sensorineural hearing loss.
In a study that came in the Egyptian Journal of Otology in 2016, by Gupta et al, about 37 cases of sudden sensorineural hearing loss were studied. They were treated with IV methyl prednisolone 2g loading dose followed by 1g BD for 2 days and then continued with oral steroids which was given in tapering doses. In that study, 24 patients had idiopathic sudden SNHL. Of this, 11 patients achieved complete recovery, whereas seven and six patients achieved partial and no recovery, respectively.12 In our study 1gm of IV methyl prednisolone was given for three days followed by tapering doses of oral steroids. PTA was repeated after completion of treatment. According to Siegel’s criteria, 5 (26%) cases showed complete recovery, 10 (52%) cases showed slight improvement and 4 (21%) cases showed no improvement. 1 case was lost to follow up. More than 30 dB hearing gain was seen in 3 patients (15%), > 15 dB hearing gain in 11 patients (55 %) and < 15 dB heaing gain was seen in 5 patients (25%). Mean improvement in hearing was found to be 19.663. Paired samples t test was done – showed that there is significant difference between pre and post PTA (p value <0.0001). This shows that steroids has a major role on treatment of ISSNHL.
Conclusion
Sudden sensorineural hearing loss is regarded as an otologic emergency, and patients are evaluated audiometrically and by an otolaryngologist on an urgent basis. It can have a devastating effect on the patient’s daily life and can be associated with a poor quality of life, even in the presence of audiological success. Known etiologies are excluded by a thorough history; physical examination; and appropriate laboratory, special audiologic, and radiologic studies. From our observations, it is clear that steroids have a positive effect on the outcome of idiopathic sudden sensorineural hearing loss. Other factors such as age or sex do not seem to have a role in the degree of hearing loss or in the post-treatment hearing improvement. Factors like the presence of vertigo or tinnitus do not seem to affect prognosis.
For idiopathic sudden sensorineural hearing loss the treatment is initial steroid therapy (as per AAO-HNS guidelines 2019). But the exact dose or route of administration of steroid is not mentioned. Our treatment protocol of initial IV pulse steroid therapy produced a recovery rate, which exceeds the spontaneous recovery rate. From our study, it is clear that initial IV pulse steroid therapy have a positive effect on the outcome of idiopathic sudden sensorineural hearing loss.
End Note
Author Information
- Dr Ihsan A.T. M.S. ENT, Professor, Department of ENT, Jubilee Mission Medical College and Research Institute, Thrissur
- Dr Vishnupriya Padmakumar, M.S ENT, DNB, Senior Resident, Department of ENT, Jubilee Mission Medical College and Research Institute, Thrissur
- Dr Prathibha Ajayakumar, M.S Department of ENT, Jubilee Mission Medical College and Research Institute, Thrissur
Conflict of Interest: None to declare
References
- Gates G A. Sudden Sensorineural Hearing Loss. In : Calais R F, Labert P R, eds. The Ear : Comprehensive Otalgia. Philadelphia, P A : Lippincott, Williams and Wilkins; 2000; 523 – 536.
[Pubmed] | [Crossref] - Schuknecht, H. F., R. S. Kimura, and P. M. Naufal. “The Pathology of Sudden Deafness.” Acta Oto-Laryngologica 76, no. 2 (1973): 75–97.
[Pubmed] | [Crossref] - Simmons FB. Theory of membrane breaks in sudden hearing loss. Archives of Otolaryngology and Head and Neck Surgery 1968; 88 : 67 – 74.
- Gussen, R. “Sudden Deafnfess of Vascular Origin: A Human Temporal Bone Study.” The Annals of Otology, Rhinology, and Laryngology 85, no. 1 Pt 1 (1976): 94–100.
[Pubmed] | [Crossref] - Byl, F. M. “Sudden Hearing Loss: Eight Years’ Experience and Suggested Prognostic Table.” The Laryngoscope 94, no. 5 Pt 1 (May 1984): 647–61.
[Pubmed] - Klemm, E., A. Deutscher, and R. Mösges. “[A present investigation of the epidemiology in idiopathic sudden sensorineural hearing loss].” Laryngo- Rhino- Otologie 88, no. 8 (August 2009): 524–27.
[Pubmed] | [Crossref] - O’Malley, Matthew R., and David S. Haynes. “Sudden Hearing Loss.” Otolaryngologic Clinics of North America 41, no. 3 (June 2008): 633–49, x–xi.
[Pubmed] | [Crossref] - Hughes, G. B., M. A. Freedman, T. J. Haberkamp, and M. E. Guay. “Sudden Sensorineural Hearing Loss.” Otolaryngologic Clinics of North America 29, no. 3 (June 1996): 393–405.
[Pubmed] - Mattox, D. E., and F. B. Simmons. “Natural History of Sudden Sensorineural Hearing Loss.” The Annals of Otology, Rhinology, and Laryngology 86, no. 4 Pt 1 (1977): 463–80.
[Pubmed] | [Crossref] - Ryan A Crane., Marc Camilon, Shaun Nguyen, and Ted A. Meyer. “Steroids for Treatment of Sudden Sensorineural Hearing Loss: A Meta-Analysis of Randomized Controlled Trials.” The Laryngoscope 125, no. 1 (January 2015): 209–17.
[Pubmed] | [Crossref] - Belhassen, S., and I. Saliba. “Intratympanic Steroid Injection as a Salvage Treatment for Sudden Sensorineural Hearing Loss.” The Journal of Laryngology and Otology 128, no. 12 (December 2014): 1044–49.
[Pubmed] | [Crossref] - Gupta V, Jain A, Banerjee PK, Rathi S. Sudden sensorineural hearing loss in adults-Our experience with a multidrug high-dose steroid regimen at a tertiary care hospital. The Egyptian Journal of Otolaryngology. 2016 Apr 1;32(2):105.